Immune checkpoint inhibitors (ICIs) have revolutionized treatment outcomes for patients with advanced non-small cell lung cancer (NSCLC); however, a fraction of patients fail to respond to ICI therapy or show no long-term benefits.1 This Phase 3 randomized trial demonstrated that administering immunochemotherapy earlier in the day (<15:00) significantly improved progression-free survival (PFS) and overall survival (OS) compared with later administration in patients with advanced non-small cell lung cancer (NSCLC). Early dosing was also associated with higher response rates and more favorable CD8+ T-cell activation profiles, without increasing toxicity. These findings suggest that time-of-day optimization represents a simple, cost-neutral strategy to enhance immunotherapy efficacy.
Study Objective
Most published clinical trials investigating ICIs have not addressed the potential influence of circadian rhythms in trial design; Circadian rhythms can significantly impact the distribution and function of immune cells, and large-scale real-world data analyses have reported better treatment outcomes with early time-of-day administration.2,3 This study aimed to prospectively evaluate whether the time (early vs. late) of day that immunochemotherapy is administered impacts clinical outcomes in patients with advanced NSCLC, specifically assessing effects on PFS, OS, and ORR.
LungTIME-C01 (Time-of-Day Immunochemotherapy in Advanced NSCLC) Study Design (NCT05549037)
- Study Design: Prospective, randomized, single-center, open-label phase 3 trial
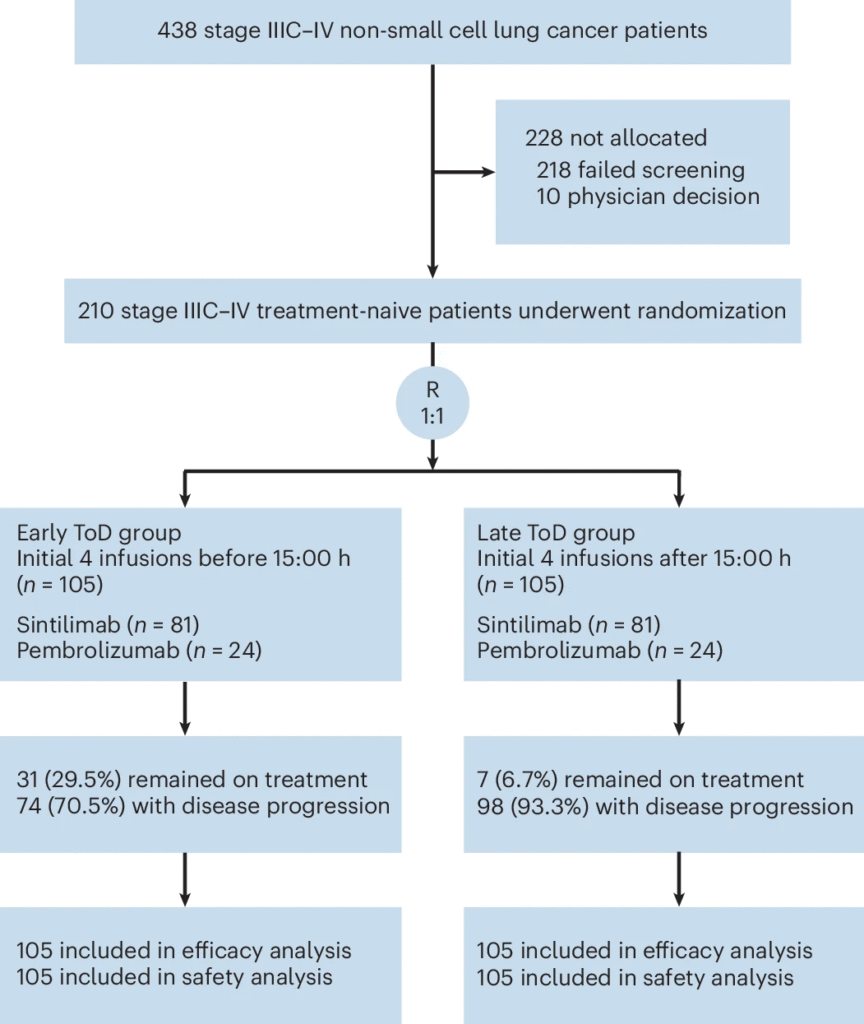
- Participants: 210 patients with treatment-naive stage IIIC-IV NSCLC without driver mutations (EGFR/ALK/ROS1)
- 190 (90.5%) – male
- 171 (81.4%) – history of smoking
- Treatment: 77.1% of patients (n=162) received sintilimab, and the remaining 22.9% (n=48) received pembrolizumab.
- Treatment Administration: Patients received chemo-immunotherapy with anti-PD-1 agents administered either early (<15:00) or late (≥ 15:00), during the first four cycles.
- Primary Endpoint: PFS
Key Efficacy Outcomes
- Primary:
- PFS: 11.3 months (early) vs. 5.7 months (late); Hazard ratio (HR) 0.40 (P<0.001)
- Secondary:
- OS: 28.0 months (early) vs. 16.8 months (late); HR 0.42 (P<0.001)
- ORR: 69.5% (early) vs. 56.2% (late) (P = 0.046)
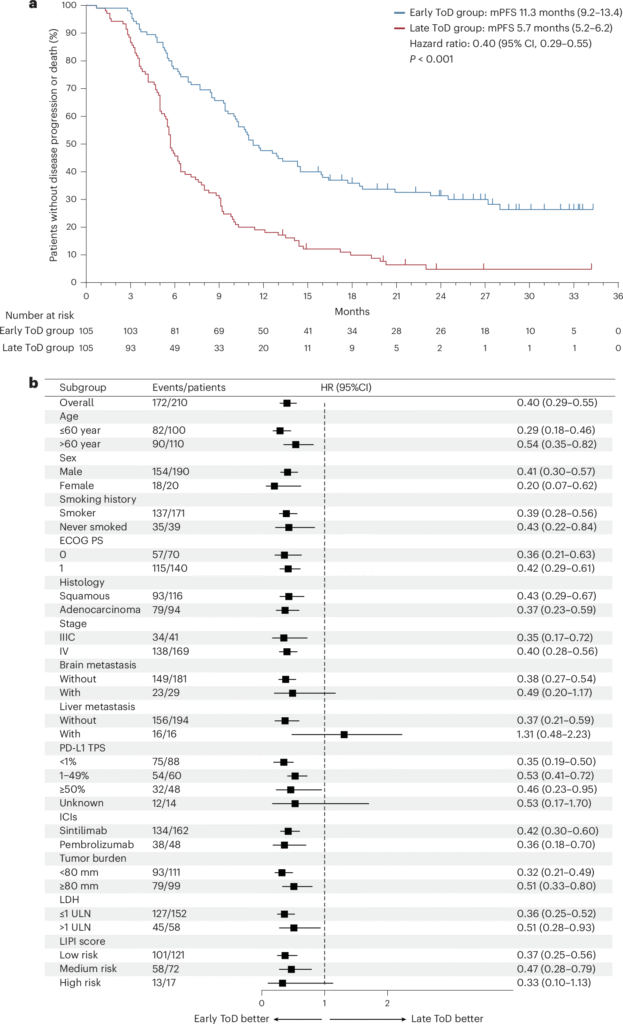
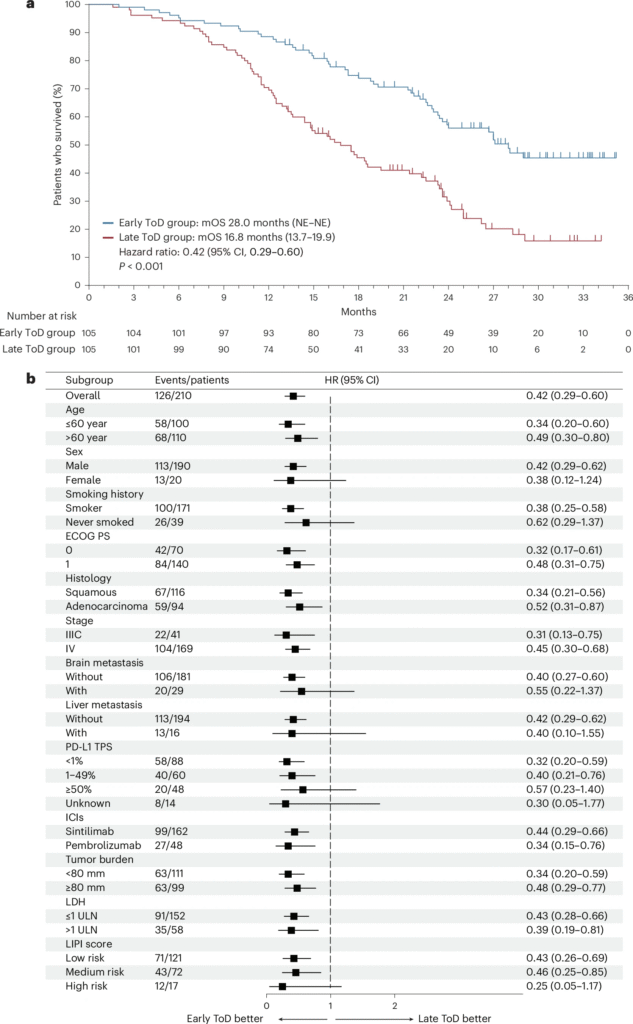
The benefit of early administration was consistent across most subgroups.
Safety
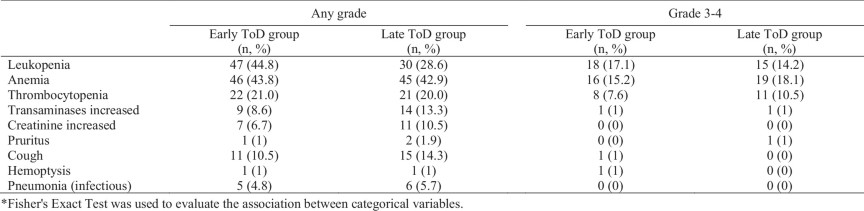
✔ No new safety signals; adverse events consistent with known profile.
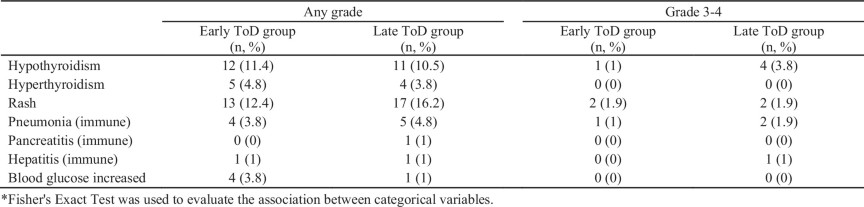
✔ No significant differences in immune-related adverse events between groups.
Mechanistic Insights
- Early time-of-day treatment is associated with:
- Increased circulating CD8+ T-cells
- Higher ratio of activated (CD8+HLA-DR+) to exhausted (TIM-3+PD-1+) CD8+ T-cells
- Suggests enhanced antitumor immune activity with earlier dosing
Conclusions
- Early time-of-day administration of immunochemotherapy significantly improves survival outcomes without added toxicity.
- This approach represents a simple, cost-neutral optimization strategy with potential implications for clinical practice and trial design.
Sources:
- Huang MY, Jiang XM, Wang BL, Sun Y, Lu JJ. Combination therapy with PD-1/PD-L1 blockade in non-small cell lung cancer: strategies and mechanisms. Pharmacol Ther. 2021;219:107694. doi:10.1016/j.pharmthera.2020.107694.
- Huang, Z., Zeng, L., Ruan, Z. et al. Time-of-day immunochemotherapy in non-small cell lung cancer: a randomized phase 3 trial. Nat Med (2026). https://doi.org/10.1038/s41591-025-04181-w.
- Huang Z, Karaboué A, Zeng L, et al. Overall survival according to time-of-day of combined immuno-chemotherapy for advanced non-small cell lung cancer: a bicentric bicontinental study. EBioMedicine. 2025;113:105607. doi:10.1016/j.ebiom.2025.105607.